Using AI to control energy for indoor agriculture
30 September 2024
Published online 1 December 2013

There is a general pessimism within the Arab society about the capacity for progress in this region. The deep political turmoil across many states curtails societies' ability to move forward. But for all the chaos, the Arab Spring did show that there are underlying forces for change, which are perhaps driving progress in unseen ways.
In various scientific fields, several countries have expanded their research capacity and productivity, and regional centres of research are thriving and growing. The expansion has seen progress in several disciplines, including HIV epidemiology. Though political and socio-cultural sensitivities surround this field of research, researchers are slowly working through these challenges, and our understanding of the epidemic has progressed to the extent that significant pieces of the HIV transmission puzzle are now in place. Yet, gaps remain.
The extent of the HIV epidemic across the region is acknowledged. In most countries, HIV infection spread among the general population is very slow, with fewer than two infected individuals for every 1000 people — one of the lowest regional rates globally.
But this overall figure masks alarming statistics. Many HIV epidemics have broken out over the last decade and they are expanding – some to alarming levels. These epidemics primarily affect high-risk and hidden populations; people who inject drugs (PWID), men who have sex with men (MSM), and female sex workers (FSWs) and their clients.
At least half of Middle East and North Africa (MENA) states are affected by HIV epidemics among MSM. In more than a third of countries in the region there are epidemics among PWID, and in a few countries there are epidemics among FSWs and their clients.
Through the interactions of these different groups with the wider population, HIV is spreading beyond the high-risk groups. For instance, HIV infections are increasing among women, most of whom are getting the virus from their spouses who engage in some high risk behaviour.
Laith Abu Raddad et al.
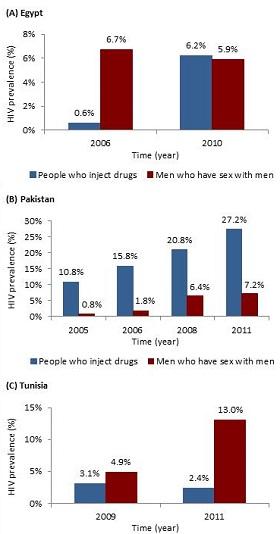
In countries such as Afghanistan, Iran, Libya, and Pakistan, HIV is mainly spreading through intravenous drug use. In Iran, Libya, and Pakistan, HIV epidemics among PWID are already at high levels. About 15% of PWID in Iran are infected. In Tripoli, Libya, 87% of PWID were found to be infected. In Pakistan, HIV prevalence among PWID has increased steadily from 11% in 2005 to 27% in 2011-2012 (Figure 1B). HIV prevalence among PWID in Egypt increased from less than 1% in 2006 to more than 6% in 2010 (Figure 1A).
The HIV epidemic among MSM and transgender populations is broader in terms of the number of countries affected, but prevalence of the virus has not reached the levels found among PWID. Across the region fewer than one in every 10 MSM is infected, but some countries are proportionately more affected. In some MSM populations, such as in Egypt, Morocco, Pakistan, Sudan, and Yemen, HIV prevalence is approaching 10%. HIV prevalence among MSM in Tunisia increased from 5% in 2009 to 13% in 2011 (Figure 1C). There are also preliminary data that indicate significant HIV epidemics among MSM in Jordan, Lebanon, and Syria, but the evidence is not yet conclusive.
HIV prevalence among FSWs is generally below 5%, and in some cases, very limited prevalence or no infections were found in sample settings. Nevertheless, FSW networks are a major driver of new HIV infections in at least several countries. In Morocco, for example, commercial heterosexual sex networks contributed about half of new HIV infections despite a low proportion of FSWs being HIV infected (2%). This significant contribution to HIV transmission is due to the larger size of these networks compared to PWID and MSM networks.
For a number of MENA countries, it appears that the core of an epidemic is limited to one part of the country. In Morocco, for instance, HIV transmission among PWID occurs mainly in the north, with limited transmission in the rest of the country, while HIV sexual transmission appears to be primarily concentrated in the southern part of the country.
In several countries, it appears that only one key at-risk population is affected by the epidemic, but this might be changing. One of the patterns over the last few years is that of the bridging of epidemics. An epidemic normally starts within one at-risk population, but, shortly after, we see another epidemic emerging among a different at-risk population within the same country.
Through evidence of overlapping risky behaviours, and often confirmed by phylogenetic analyses of the virus subtypes, it appears that the second epidemic has its roots in the first one. The rising epidemic among MSM in Pakistan, which began shortly after the emergence of the epidemic among PWID, provides an example of this pattern (Figure 1).
This bridging of epidemics also appears to happen across national boundaries. The HIV epidemics among PWID in Afghanistan, Iran, and Pakistan, appear to be linked with the virus apparently crossing borders through the drug trade routes and refugee movements. The epidemic started in Iran, moved to Pakistan, and a few years later became evident in Afghanistan after the return of Afghan refugees from Iran.
Monitoring of HIV epidemics in MENA is very uneven across different countries. A recent assessment showed that only four out of 23 MENA countries had effective HIV surveillance systems capable of tracking the epidemics. Several countries, such as Afghanistan, Djibouti, Egypt, Jordan, Lebanon, Libya, Somalia, Sudan, Tunisia, and Yemen, have made major strides in identifying and analyzing their HIV epidemics.
Few countries not only now understand their epidemics, but have also developed a strong HIV response that makes a difference in combatting transmission. Iran is one such country with an admirable response towards their HIV epidemic among PWID. Morocco is also MENA's most outstanding country in confronting the epidemic through an evidence-based, enlightened, and comprehensive response.
However, a number of countries continue to lag far behind in their understanding of epidemics and their HIV response. This is of grave concern because there are indirect data suggesting the emergence of significant hidden HIV epidemics among the key populations at risk in some of these states.
Globally, the HIV epidemic is in a declining trend, but not so in MENA. The epidemic, slow-growing for decades, is now expanding with multiple epidemics emerging among the key at-risk populations across the MENA region. Though our knowledge is still limited to a number of countries, several countries have a clear picture, and, in a few instances, are combatting the epidemic through evidence-informed approaches.
Though most public health policymakers in MENA realize that the epidemic is a reality within their countries, this realization is yet to be translated into coherent and relevant action in most states.
Laith J. Abu-Raddad is an associate professor of Public Health, and Hiam Chemaitelly and Ghina R. Mumtaz _ are research specialists, at the Infectious Disease Epidemiology Group at Weill Cornell Medical College in Qatar.
Funding Acknowledgment This article was made possible by NPRP grant number 4-924-3-251 from the Qatar National Research Fund (a member of Qatar Foundation). The statements made herein are solely the responsibility of the authors.
doi:10.1038/nmiddleeast.2013.229
30 September 2024
23 September 2024
11 September 2024
Sign-up to receive our e-alert update every two weeks to keep up with everything new on the portal.
Sign up for e-alerts
Stay connected: