Using AI to control energy for indoor agriculture
30 September 2024
Published online 17 March 2016
As the Zika virus makes its mark in the Americas, what is the risk of it taking hold in the Middle East and North Africa?

© James Gathany
Since its appearance on Easter Island off the pacific coast of Chile in February 2014, the virus has rampaged across the Americas and is now spreading beyond it. Although the Middle East is not the ideal habitat for A. aegypti, the region’s geographic position and limited systemic capacity to respond quickly to viral threats, mean health authorities should be on alert.
As of early March, 2016, transmission has been recorded domestically in 31 countries and territories in the Americas, in the Pacific Islands, Cape Verde near the coast of West Africa, Gabon, and multiple countries in Southeast Asia. In the Americas alone, the World Health Organization (WHO) expects the outbreak to result in 3-4 million infections over the coming year.
Clinically, Zika virus patients usually have no symptoms, and those that do present are limited to fever, rash, joint pain, and conjunctivitis and normally last a few days to a week. Such symptoms are nonspecific — and are caused by a number of mosquito-transmitted viruses including dengue.
The vast majority of those infected recover without problems.
Of graver concern with Zika now, though, is its possible connection to more than 5,000 reported cases of congenital microcephaly and hundreds of new cases of Guillain-Barré syndrome (GBS) in the region.
Microcephaly is a potentially serious neurodevelopmental disorder in infants and is defined by an abnormally small head circumference. Often this indicates underdevelopment or malformation of the brain, which in turn carries the possibility of lifelong developmental disability.
GBS, on the other hand, usually affects adults. In this condition, Zika virus infection may trigger the body’s own immune system to attack the nervous system resulting in temporary paralysis that can encumber the ability to breathe. Although usually lasting a few weeks to months, approximately 5% of people affected by GBS in the past have died.
On February 1, 2016, the WHO officially declared the Zika virus outbreak a Public Health Emergency of International Concern, calling for rapid scale-up of research efforts to understand the etiology of the many microcephaly and GBS cases and their putative relationship to Zika virus. The US Centers for Disease Control and Prevention has recommended pregnant women avoid travel to affected countries, and several Latin American countries have taken the extraordinary step of recommending women postpone pregnancy for up to two years to reduce the risk of fetal complications.
Without a vaccine or specific treatment for Zika virus infection, control of the outbreak currently hinges on reducing the Aedes population with insecticides and by removing stagnant water where the mosquitoes breed — a daunting task given the mosquito’s adaptation to urban environments and its ability to reproduce in water containers the size of a bottle cap.
Zika virus and implications for the Middle East and North Africa
© John Humphrey
Enlarge image
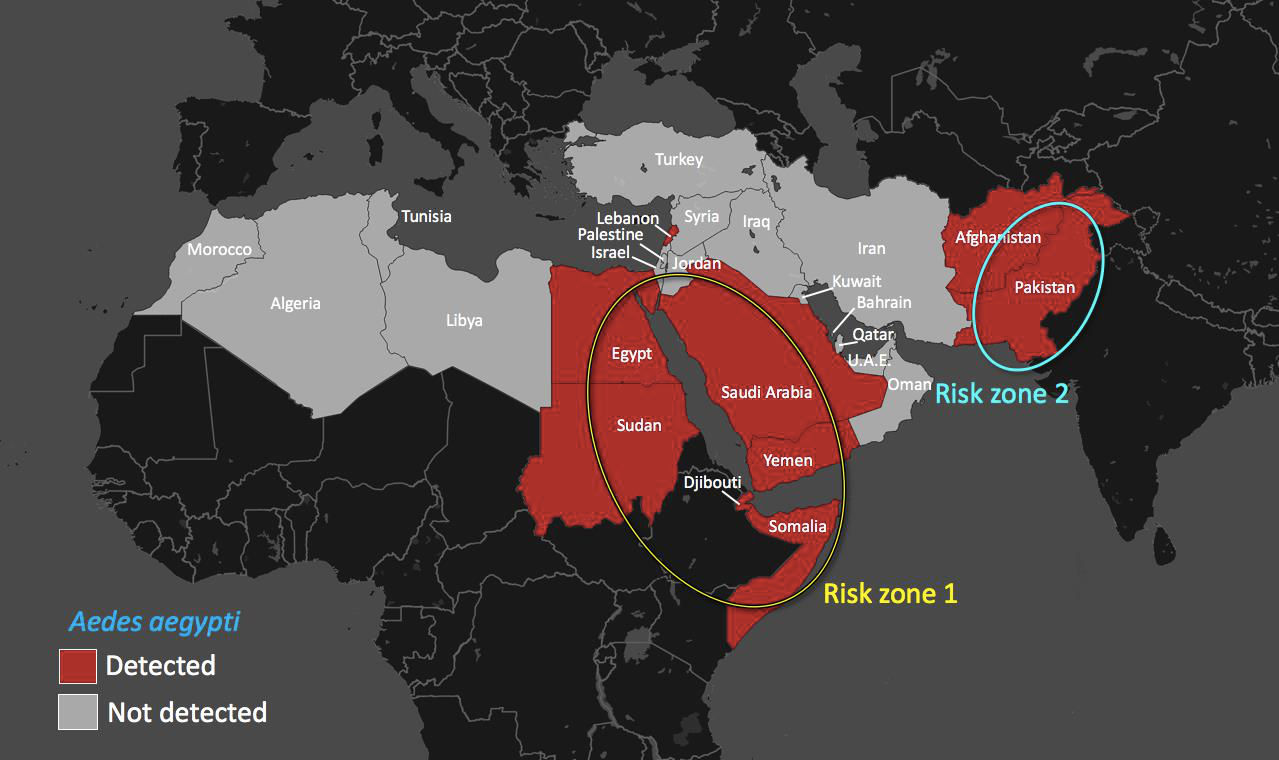
Hence, the geographic distribution of A. aegypti in the region is key to predicting the distribution of the viruses it carries, including dengue, Chikungunya, and yellow fever (see map).
Aedes distribution is in turn dependent on a range of ecologic factors including temperature and rainfall — making much of the Middle East and North Africa poorly suited for Aedes inhabitation.
Still, certain areas of the Middle East and North Africa are proving increasingly capable of sustaining Aedes-borne virus transmission.
Multiple outbreaks of dengue have been reported along the Red Sea coasts of Sudan, Djibouti, Somalia, Yemen, and Saudi Arabia.
In Saudi Arabia, dengue infections reached an all-time high in 2013 with more than 4,400 reported cases. Dengue cases have climbed in Yemen as well, with more than 3,000 cases in the summer of 2015 as the spread of the virus was aided by the country’s ongoing humanitarian crisis and collapsing public health infrastructure.
In 2011, a Chikungunya virus outbreak that ignited in Yemen and Saudi Arabia claimed over 15,000 suspected cases. This outbreak was the first ever recorded local transmission of Chikungunya virus in the Arabian Peninsula — but it is unlikely to be the last.
In Egypt, widespread dengue transmission was reported for years before large scale insecticide campaigns in the 1940s reduced the A. aegypti population. Dengue resurfaced in October 2015, however, in an A. aegypti-driven outbreak along the Nile river in Upper Egypt that yielded 253 cases. Even yellow fever, the only Aedes-transmitted virus for which there is a licensed vaccine, has resurged in Sudan. A 2012 outbreak in Darfur was declared the worst to occur in the world in decades.
To make matters worse, many of the Middle East and North African countries affected by Aedes-transmitted viruses are among the poorest in the region, least equipped to recognize and respond quickly to outbreaks when they occur and to provide adequate health care to patients. Their health-care systems have limited resources and are already severely strained.
On January 28th, the Assistant Director-General for the WHO advised that “any country in the dengue belt that has Aedes aegypti should be looking at whether there is Zika and put in place measures to detect neurological conditions.”
In Aedes endemic countries surrounding the Red Sea (see figure, risk zone 1) and Pakistan (risk zone 2), the potential is certainly there.
However, the low volume of travelers arriving from Zika-endemic countries, and the short duration of viremia (e.g. the period of infectivity) of usually 3-5 days, makes introduction of Zika virus in these risk zones difficult.
Still, cases have been reported in travelers returning to the US, UK, China, and South Africa in recent weeks, and the millions of people from around the world that will gather in September for the Hajj in Mecca, an A. aegypti endemic area with previous dengue outbreaks, raises genuine concern.
Through much of the Middle East and North Africa, surveillance for vector-borne infections like dengue and Chikungunya remains limited and the distribution of A. aegypti remains insufficiently characterized.
The story of Zika virus thus carries an important lesson for the region: emerging vector-borne infections pose a present threat to Aedes-endemic countries, and the need to analyze the distribution of A. aegypti and prevent its spread throughout the region has never been more urgent.
John Humphrey is a Fellow in Infectious Diseases at Weill Cornell Medical College, Cornell University. Marshall Glesby is a Professor of Medicine at Weill Cornell Medical College, Cornell University. Laith Abu-Raddad is an Associate Professor of Healthcare Policy and Research at the Weill Cornell Medical College – Qatar, Cornell University.
This commentary was based on research work conducted by John Humphrey through support from NIH Research Training grant T32 AI007613.doi:10.1038/nmiddleeast.2016.35
30 September 2024
23 September 2024
11 September 2024
Sign-up to receive our e-alert update every two weeks to keep up with everything new on the portal.
Sign up for e-alerts
Stay connected: