The Missing Kingdom: Why Fungi Must Be Central to Conservation Strategy
28 December 2025
Published online 3 April 2020
Nature Middle East asked Ghina Mumtaz1 , an epidemiologist working in Lebanon, about the spread of COVID-19 in the Arab region.

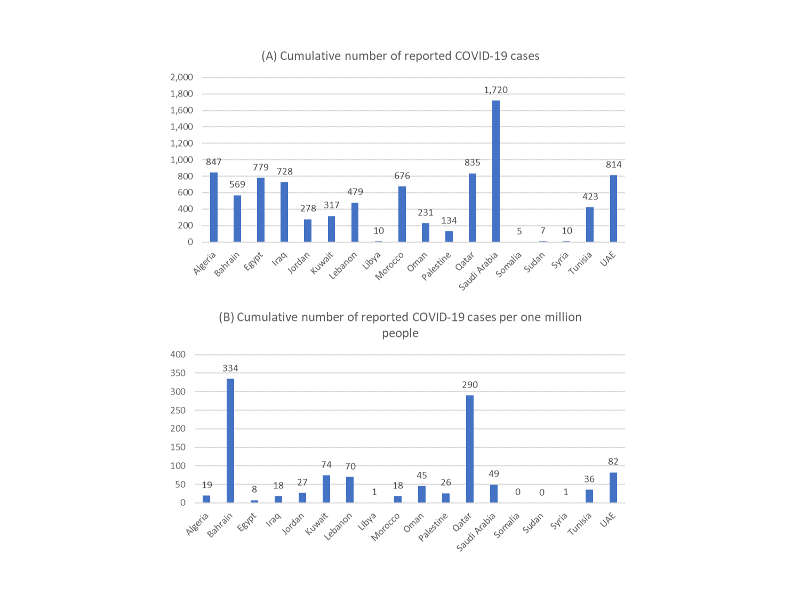
Another potential explanation for these currently smaller numbers could be the lower levels of testing and reporting in some Arab countries. Lower income countries will not have sufficient resources to scale up testing, will have limited laboratory capacity, and weak surveillance systems. This means there might be undocumented transmission. Differentials in testing are observed even within regions and are usually linked to available resources. For example, many of the Arab Gulf countries, such as the UAE, Bahrain, and Qatar, rank among the highest in the world in terms of the number of tests per one million population, while the rest of the Arab world has conducted little testing, comparatively. It is not surprising that these three countries have the highest number of reported cases per one million inhabitants in the region (figure).
There is a lot of speculation about the potential effect of seasonality and warmer weather on the spread of the virus, with some arguing that the epidemic has not spread much in the African continent because of warmer weather. However, the effect of seasonality is still not known. Even if warmer weather might slow the spread of the infection, it is unlikely that, alone, this could prevent an epidemic from happening. This is especially applicable in the case of SARS-CoV-2 infection, the virus causing COVID-19, due to its high reproduction number (R0) of about 2.5, compared with seasonal influenza’s R0 of about 1.3. The reproduction number is the average number of secondary infections caused by one infected person at the beginning of an epidemic. It provides an indication of the intrinsic potential of an infectious agent to spread in a given population.
Ghina Mumtaz
Enlarge image
Finally, while mortality is affected by the quality of care, the currently observed low death rates in some Arab countries might be explained by the protective effect of age. Based on published epidemiological evidence, the severity of COVID-19 has strong links to advanced age. The proportion of cases who develop severe or critical disease increases steadily with age. The demographic profile in developed countries, in terms of age structure, is very different compared to developing countries. The latter, including most of the Arab world, have much younger populations, and could be expected to have less critical disease cases and hence lower mortality. Italy, which has documented a high death toll, has one of the oldest populations in the world. However, one has to keep in mind that it could take up to eight weeks following the initial onset of symptoms before people develop critical complications and death.
Since the infections in Arab countries could be lagging behind those in other regions, it may be premature to think that mortality is low in this part of the world.
doi:10.1038/nmiddleeast.2020.45
28 December 2025
24 December 2025
24 December 2025
02 April 2020
17 March 2020
18 March 2020
Sign-up to receive our e-alert update every two weeks to keep up with everything new on the portal.
Sign up for e-alerts
Stay connected: